Decision making support for nurses and health workers, even when connectivity is poor or low, is possible with Sana Mobile, an Android-based mobile health application. Formerly known as Moca Mobile, the Sana technology facilitates remote consultations between health care specialists and community health workers in remote areas.
Sana Mobile started at MIT's NextLab, where developers, faculty and students collaborate to tackle a problem using mobile technology. The Sana technology was developed by Sidhant Jena, Sana team lead and Harvard Business School student and Russell Ryan, lead engineer and MIT student.
When general practitioners lack the expertise to diagnose a case, they refer patients to specialists, who may not be easily accessible. The Sana technology addresses the lack of accessibility to specialty care in places, where specialist doctors and tertiary care centers are sparse.
How does Sana Mobile work?
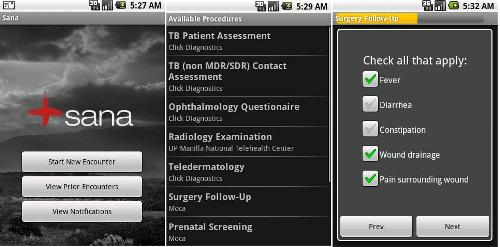
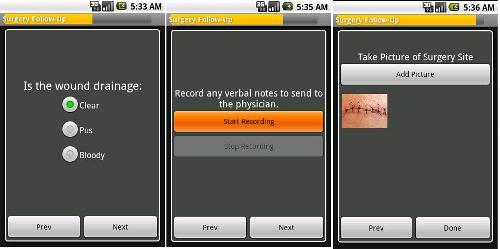
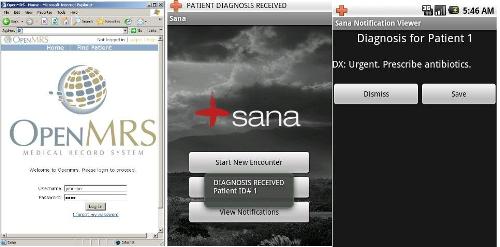
Using Sana, physicians can create medical procedures and upload them to phones used by health workers and nurses. Procedures are step-by-step instructions that guide the community health worker through all the data points that need to be collected and questions that need to be asked during an appointment with a patient. Health workers can run these pre-programmed medical procedures on their phones and collect the required patient data, including pictures and video as they are prompted. The information collected can be uploaded to a web-based medical health record system for a doctor to review. The diagnosis or recommendation for follow-up is sent back to the community health worker, who then communicates this information back to the patient.
Sana improves accessibility to specialist care for geographically isolated patients
We spoke to Sayon Dutt, a member on the Sana Operations team, who described the ways Sana could be used. Patients living in remote areas, who experience pain or swelling from a surgical wound may have to travel far distances to reach a specialist, often to urban centers. If patients do not follow-up nor seek help, they put themselves at a higher risk of complication. By integrating voice, text, picture and video in the data collection process, health workers, primary care physicians and nurses, who may have limited expertise, can remotely consult with specialists in urban areas.
He added that while in small clinics the technology to take ultrasound and x-rays may exist, the medical radiology skills to interpret the images may be lacking. High resolution pictures of an x-ray image or ultrasound image can be taken and sent to specialists for instant feedback as well. (See screenshots of the Sana workflow below).
Sana integrates with existing health care technology, creates efficiences in work flow management and works over unreliable networks!
Sayon explained, “Sana Mobile empowers the community health worker to act as a conduit for the surgeon or doctor and helps the patient receive expedited medical care, without having to travel far.”
The Sana application is fully compatible with OpenMRS, an open source medical records system, but can also integrate with other medical records systems being used. (See this link to see how it integrates with OpenMRS) This is why Sana Mobile is heralded as an end-to-end decision making support tool that assists in streamlining work flow.
For common medical procedures, physicians can also create decision trees to increase efficiencies in making diagnoses. Sana’s branching feature allows a final diagnosis to be displayed based on the answers a health worker chooses within a given procedure. This removes the need for community health workers to wait for a doctor’s review, and saves time if there are connectivity limitations.
An interesting feature is Sana’s synchronization, packetization and multimodal transfer abilities. There are built-in features that allow data to be transferred over unreliable networks.
- Synchronization: Completed forms are stored locally on the phone. So, while new procedures are being filled, the phone is constantly searching for cellular service to upload the ones that are completed.
- Packetization: Video and high-resolution images are uploaded in chunks over GPRS, to accommodate for unreliable connections.
- Multi-modal transfers: Data is transferred using multiple interfaces, including GPRS, WiFi, SMS and USB cable depending on the size and quality of data. Images and sounds are transferred on GPRS, WiFi or USB. Text filled out in a procedure and physicians’ responses and diagnoses are sent via SMS.
Work flow of a CHW using Sana Mobile and Doctor's feedback and diagnosis
Putting Sana to the test: Oral Cancer Screening in India
Oral cancer is one of the most common cancers in India. It is related to the cultural practice of chewing paan masala and gutka. It is estimated that about 40% of men and 15% of women chew tobacco on a regular basis. Detecting risk of oral cancer earlier is important for affordable treatment as late stage tumors can be very expensive to treat.
Dr. Moni Kuriakose, project lead at Narayana Hrudayalaya, a large cardiac hospital in Bangalore, said recently in an interview with the Hindu:
‘Most patients at our hospitals show up with stage-4 tumours that cost lakhs [of rupees] to treat and the survival [rate] is 30 per cent. If detected early, the survival rates go up to 90 per cent and cost Rs 15,000-30,000 to treat.’
To survey the risk of oral cancer in their community, Mazumdar Shaw Cancer Center and the Narayana Hrudayalaya Health to ran a pilot test in and around Bangalore over six months. One pilot was run in Belgaum, Raichur, a rural town about 12 hours away from the city of Bangalore. The other pilot was run in Bangalore. Equipped with the Sana application, ASHAs (community health workers) went door to door in and around Bangalore, asking questions and taking pictures of oral lesions, which were evaluated by oral surgeons. In six months, they were able to screen about 400 high-risk cancer patients and detected numerous lesions using Sana. Twenty ASHAs were trained in using the Sana software in Belgaum.
Dr. Paul Salins, the Medical Director of the MSCC spoke with the Hindu, about opportunities for scaling:
“In the next few months, we will be scaling this to other medical institutions within the State and hopefully by next year [2011] cover other chronic diseases such as heart disease, diabetes and chronic kidney disease.”
For any project using Sana, the team always tries to enable local stakeholders. Sana invests in local champions, training them to do basic development of the system. Technical familiarity with Android, and OpenMRS is recommended. “If you don’t have local buy-in, there’s no real long-term sustainability answer,” said Sayon.
In Bangalore, the Sana Team observed nurses in a surgery ward during their rounds. After nurses checked on patients, using a paper based form, they would call the doctor to describe the status of each patient over the phone. The paper forms are filed, but often misplaced. Sana can remove these redundancies and create efficiencies. Doctors could monitor their patients from their office on the web-based registry, and forms could be automatically filed in the patients’ electronic medical records.
Sayon talked about the challenges that come with introducing a new technology into a resource limited region. Changes in work flow management can be met with resistance. Physicians are accustomed in doing their work in a certain way, and not necessarily willing to change or learn how to use the internet to review cases. Physicians are critical stakeholders that need to be engaged for successful adoption of such technology.
Adaptions needed to happen in the field for better usability
Russell Ryan, the lead engineers for Sana, visited India to test the technology. He spoke about the challenges faced in the Bangalore pilot. One of the biggest problems faced in Raichur was with respect to language. Some health workers in Raichur were not literate in Kannada, the local script, or English. Unfortunately, the Android platform does not currently support every language script in the world. The Sana application is currently only available in English, Spanish and Chinese. In Bangalore, the Sana developers tweaked the system to replace text prompts with voice prompts, to take pictures or video. They also added pictorial labels, using forward and back arrows, instead of the text “next” and “previous” to display navigation between forms.
With respect to the usability of the phone, Russell observed that health workers initially experienced challenges in using the touch screen. The users were not familiar with this type of computer interface, and had not yet learned where to touch and how. This was solved with additional training and familiarity.
Sana will also be used to conduct a risk assessment for cardiovascular disease in Punjab. In this project, run by E-Health Points, health workers will go door to door to survey risk factors. For these pilots, the team is developing an algorithm based on data entered for instant feedback to the health worker of a patient’s level of risk.
Android based m-health platforms is the new future?
Budget for Sana deployments has primarily been limited by the cost of the phone. Currently, Sana only runs on Android enabled phones, which may be expensive, and prohibitive. Sana developers believe that there are already many low-cost systems for basic mobile phones that are running quite successfully. But they wanted to develop a mobile phone based health care application that offers the ability to use the full capabilities of the phone.
They turned to Android to be able to integrate high quality pictures and video capabilities for improved decision support to get a fuller picture of a patient’s condition. This is especially important for specialized, complicated cases as in follow-ups after surgery or diagnostic imaging.
The team is interested in importing to cheaper Nokia handsets in the future. But equally are optimistic about Google’s announcement to introduce a $200 handset, which may reduce concerns regarding cost.
Sana Mobile is an open source application. The code can be downloaded here, and instructions and How-Tos can be found on the Sana wiki page. See here for more Sana demos.
Sana Mobile: Connecting Big-City Care to Patients in Remote Villages Locations
Decision making support for nurses and health workers, even when connectivity is poor or low, is possible with Sana Mobile, an Android-based mobile health application. Formerly known as Moca Mobile, the Sana technology facilitates remote consultations between health care specialists and community health workers in remote areas.
Sana Mobile started at MIT's NextLab, where developers, faculty and students collaborate to tackle a problem using mobile technology. The Sana technology was developed by Sidhant Jena, Sana team lead and Harvard Business School student and Russell Ryan, lead engineer and MIT student.
When general practitioners lack the expertise to diagnose a case, they refer patients to specialists, who may not be easily accessible. The Sana technology addresses the lack of accessibility to specialty care in places, where specialist doctors and tertiary care centers are sparse.
How does Sana Mobile work?
Using Sana, physicians can create medical procedures and upload them to phones used by health workers and nurses. Procedures are step-by-step instructions that guide the community health worker through all the data points that need to be collected and questions that need to be asked during an appointment with a patient. Health workers can run these pre-programmed medical procedures on their phones and collect the required patient data, including pictures and video as they are prompted. The information collected can be uploaded to a web-based medical health record system for a doctor to review. The diagnosis or recommendation for follow-up is sent back to the community health worker, who then communicates this information back to the patient.
Sana improves accessibility to specialist care for geographically isolated patients
We spoke to Sayon Dutt, a member on the Sana Operations team, who described the ways Sana could be used. Patients living in remote areas, who experience pain or swelling from a surgical wound may have to travel far distances to reach a specialist, often to urban centers. If patients do not follow-up nor seek help, they put themselves at a higher risk of complication. By integrating voice, text, picture and video in the data collection process, health workers, primary care physicians and nurses, who may have limited expertise, can remotely consult with specialists in urban areas.
He added that while in small clinics the technology to take ultrasound and x-rays may exist, the medical radiology skills to interpret the images may be lacking. High resolution pictures of an x-ray image or ultrasound image can be taken and sent to specialists for instant feedback as well. (See screenshots of the Sana workflow below).
Sana integrates with existing health care technology, creates efficiences in work flow management and works over unreliable networks!
Sayon explained, “Sana Mobile empowers the community health worker to act as a conduit for the surgeon or doctor and helps the patient receive expedited medical care, without having to travel far.”
The Sana application is fully compatible with OpenMRS, an open source medical records system, but can also integrate with other medical records systems being used. (See this link to see how it integrates with OpenMRS) This is why Sana Mobile is heralded as an end-to-end decision making support tool that assists in streamlining work flow.
For common medical procedures, physicians can also create decision trees to increase efficiencies in making diagnoses. Sana’s branching feature allows a final diagnosis to be displayed based on the answers a health worker chooses within a given procedure. This removes the need for community health workers to wait for a doctor’s review, and saves time if there are connectivity limitations.
An interesting feature is Sana’s synchronization, packetization and multimodal transfer abilities. There are built-in features that allow data to be transferred over unreliable networks.
- Synchronization: Completed forms are stored locally on the phone. So, while new procedures are being filled, the phone is constantly searching for cellular service to upload the ones that are completed.
- Packetization: Video and high-resolution images are uploaded in chunks over GPRS, to accommodate for unreliable connections.
- Multi-modal transfers: Data is transferred using multiple interfaces, including GPRS, WiFi, SMS and USB cable depending on the size and quality of data. Images and sounds are transferred on GPRS, WiFi or USB. Text filled out in a procedure and physicians’ responses and diagnoses are sent via SMS.
Work flow of a CHW using Sana Mobile and Doctor's feedback and diagnosis
Putting Sana to the test: Oral Cancer Screening in India
Oral cancer is one of the most common cancers in India. It is related to the cultural practice of chewing paan masala and gutka. It is estimated that about 40% of men and 15% of women chew tobacco on a regular basis. Detecting risk of oral cancer earlier is important for affordable treatment as late stage tumors can be very expensive to treat.
Dr. Moni Kuriakose, project lead at Narayana Hrudayalaya, a large cardiac hospital in Bangalore, said recently in an interview with the Hindu:
‘Most patients at our hospitals show up with stage-4 tumours that cost lakhs [of rupees] to treat and the survival [rate] is 30 per cent. If detected early, the survival rates go up to 90 per cent and cost Rs 15,000-30,000 to treat.’
To survey the risk of oral cancer in their community, Mazumdar Shaw Cancer Center and the Narayana Hrudayalaya Health to ran a pilot test in and around Bangalore over six months. One pilot was run in Belgaum, Raichur, a rural town about 12 hours away from the city of Bangalore. The other pilot was run in Bangalore. Equipped with the Sana application, ASHAs (community health workers) went door to door in and around Bangalore, asking questions and taking pictures of oral lesions, which were evaluated by oral surgeons. In six months, they were able to screen about 400 high-risk cancer patients and detected numerous lesions using Sana. Twenty ASHAs were trained in using the Sana software in Belgaum.
Dr. Paul Salins, the Medical Director of the MSCC spoke with the Hindu, about opportunities for scaling:
“In the next few months, we will be scaling this to other medical institutions within the State and hopefully by next year [2011] cover other chronic diseases such as heart disease, diabetes and chronic kidney disease.”
For any project using Sana, the team always tries to enable local stakeholders. Sana invests in local champions, training them to do basic development of the system. Technical familiarity with Android, and OpenMRS is recommended. “If you don’t have local buy-in, there’s no real long-term sustainability answer,” said Sayon.
In Bangalore, the Sana Team observed nurses in a surgery ward during their rounds. After nurses checked on patients, using a paper based form, they would call the doctor to describe the status of each patient over the phone. The paper forms are filed, but often misplaced. Sana can remove these redundancies and create efficiencies. Doctors could monitor their patients from their office on the web-based registry, and forms could be automatically filed in the patients’ electronic medical records.
Sayon talked about the challenges that come with introducing a new technology into a resource limited region. Changes in work flow management can be met with resistance. Physicians are accustomed in doing their work in a certain way, and not necessarily willing to change or learn how to use the internet to review cases. Physicians are critical stakeholders that need to be engaged for successful adoption of such technology.
Adaptions needed to happen in the field for better usability
Russell Ryan, the lead engineers for Sana, visited India to test the technology. He spoke about the challenges faced in the Bangalore pilot. One of the biggest problems faced in Raichur was with respect to language. Some health workers in Raichur were not literate in Kannada, the local script, or English. Unfortunately, the Android platform does not currently support every language script in the world. The Sana application is currently only available in English, Spanish and Chinese. In Bangalore, the Sana developers tweaked the system to replace text prompts with voice prompts, to take pictures or video. They also added pictorial labels, using forward and back arrows, instead of the text “next” and “previous” to display navigation between forms.
With respect to the usability of the phone, Russell observed that health workers initially experienced challenges in using the touch screen. The users were not familiar with this type of computer interface, and had not yet learned where to touch and how. This was solved with additional training and familiarity.
Sana will also be used to conduct a risk assessment for cardiovascular disease in Punjab. In this project, run by E-Health Points, health workers will go door to door to survey risk factors. For these pilots, the team is developing an algorithm based on data entered for instant feedback to the health worker of a patient’s level of risk.
Android based m-health platforms is the new future?
Budget for Sana deployments has primarily been limited by the cost of the phone. Currently, Sana only runs on Android enabled phones, which may be expensive, and prohibitive. Sana developers believe that there are already many low-cost systems for basic mobile phones that are running quite successfully. But they wanted to develop a mobile phone based health care application that offers the ability to use the full capabilities of the phone.
They turned to Android to be able to integrate high quality pictures and video capabilities for improved decision support to get a fuller picture of a patient’s condition. This is especially important for specialized, complicated cases as in follow-ups after surgery or diagnostic imaging.
The team is interested in importing to cheaper Nokia handsets in the future. But equally are optimistic about Google’s announcement to introduce a $200 handset, which may reduce concerns regarding cost.
Sana Mobile is an open source application. The code can be downloaded here, and instructions and How-Tos can be found on the Sana wiki page. See here for more Sana demos.

Post new comment